The surgical team performed external fixation of the right femur, followed by debridement and irrigation of Masooma K.’s lower extremities, followed by a completion amputation to the viable level of her left lower extremity, above the knee.
“I debated limb salvage versus completion amputation to the patient’s right lower extremity. While my partners were working on her abdomen and I was completing her left leg amputation, the patient began to have difficulty ventilating and displayed tension physiology, so we placed a second chest tube.”
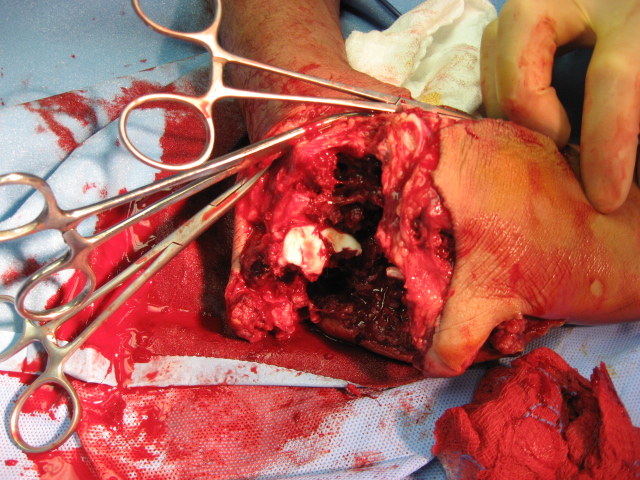
“We began to have trouble keeping the patient’s blood pressure stable. Her abdomen became edematous after her intestinal repairs, so I elected to amputate her right lower extremity at a very distal ankle disarticulation.” Masooma K. survived the night and stabilized later postop day 1, enough for aeromedical critical care transportation to a higher echelon facility.

1. Was there any real role for limb salvage in an austere environment, given that this patient would be transferred to a higher level hospital within 24 hours?
2. Is there any difference between a Syme amputation vs. a low transtibial amputation vs. a below-knee amputation in countries supported solely by the International Committee of the Red Cross for prosthetics?
3. What is the fate of a female double amputee in Afghanistan?